

The EMCDDA has released today a new miniguide on drug consumption rooms (DCR) as part of its Health and social responses to drug problems: a European guide. The resource is the first miniguide in a bundle of reports dedicated to drug-related interventions. It provides an overview of key issues related to these facilities, including service delivery, guidance and existing evidence and latest developments in Europe. It also considers implications for policy and practice.
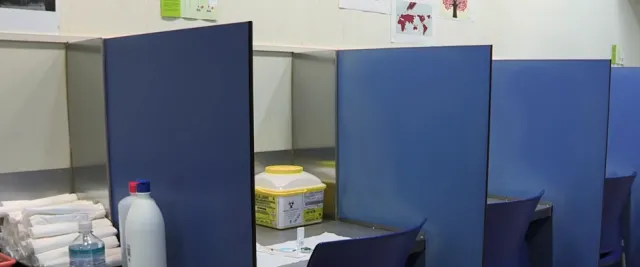
DCRs are professionally supervised healthcare facilities (fixed or mobile) where people who use drugs can do so under safer and more hygienic conditions. They generally aim to address a mix of individual health, public health and public order objectives and to reach out to the most marginalised populations.
Primarily, DCRs aim to prevent drug-related overdose deaths, reduce the acute risks of disease transmission through unhygienic injecting, and connect people who use drugs with addiction treatment and other health and social services. Their main source of funding is usually local government.
These facilities are usually located in areas near open drug scenes and where injecting in public places is common. As frontline, low-threshold services, DCRs can play a role in the early identification of new and emerging trends among high-risk populations using their services.
In the context of today's dynamic drugs problem, DCRs are adapting their services to local client needs and drug market trends by addressing a broad range of practices and harms. This has included providing services for smoking as well as injecting and allowing the consumption of a wider range of substances within the facility.
According to the miniguide, DCRs vary in organisation, staffing and service delivery reflecting both the availability of resources and the needs of the communities in which they are located, as well as local regulatory approaches.
The miniguide identifies two main operational models of service delivery for DCRs in Europe. These are: integrated DCRs, operating within low-threshold facilities (e.g. healthcare or harm reduction centres, overnight shelters) where the supervision of drug use is just one of the services offered; and specialised DCRs, offering a narrower range of services directly related to supervised consumption. Mobile DCRs also exist to reach more dispersed populations or in cases of local resistance to fixed sites.
The geographical distribution of drug consumption rooms is uneven, both at the international and regional levels. More than 100 DCRs are in operation globally, with services in Europe, Australia, Canada, Mexico and the United States. In Europe, DCRs have been operating since 1986, when the first was established in Bern, Switzerland. Since then, such facilities have been opened in cities in an increasing number of European countries, including Belgium, Denmark, France, Germany, Greece, Iceland, Luxembourg, the Netherlands, Norway, Portugal and Spain (see map).
As services, DCRs are particularly challenging to evaluate. This means generalising from the existing research evidence in this area is difficult. Currently available evidence suggests that DCRs may have a beneficial effect on a number of outcomes. These include:
- improving access to healthcare and harm reduction services for hard-to-reach target populations;
- reducing drug-related deaths;
- reducing injecting risk behaviours;
- reducing drug use in public spaces and alleviating overall public nuisance in areas in which high levels of public drug use occur.
The guide concludes that more studies are needed to improve the body of evidence available on the effectiveness of DCRs in reducing harms at the individual and community levels.
Among other measures to reduce cases of fatal and non-fatal overdose, the EU Drugs Action Plan 2021–2025 calls for DCRs to be introduced, maintained or enhanced 'where appropriate and in accordance with national legislation'.